Joint strategic needs assessment
Tobacco control (2020)
This is an online synopsis of the topic which shows the executive summary and key contacts sections. To view the full document, please download it.
| Topic title | Tobacco control (2020) |
|---|---|
| Topic owner | Virtual Tobacco Task & Finish Group |
| Topic author(s) | Daniel Youhana & Jo Marshall |
| Topic quality reviewed | October 2019 |
| Topic endorsed by | Virtual Tobacco Task & Finish Group |
| Topic approved by | Health and Wellbeing Board January 2020 |
| Current version | January 2020 |
| Replaces version | 2015 |
Executive summary
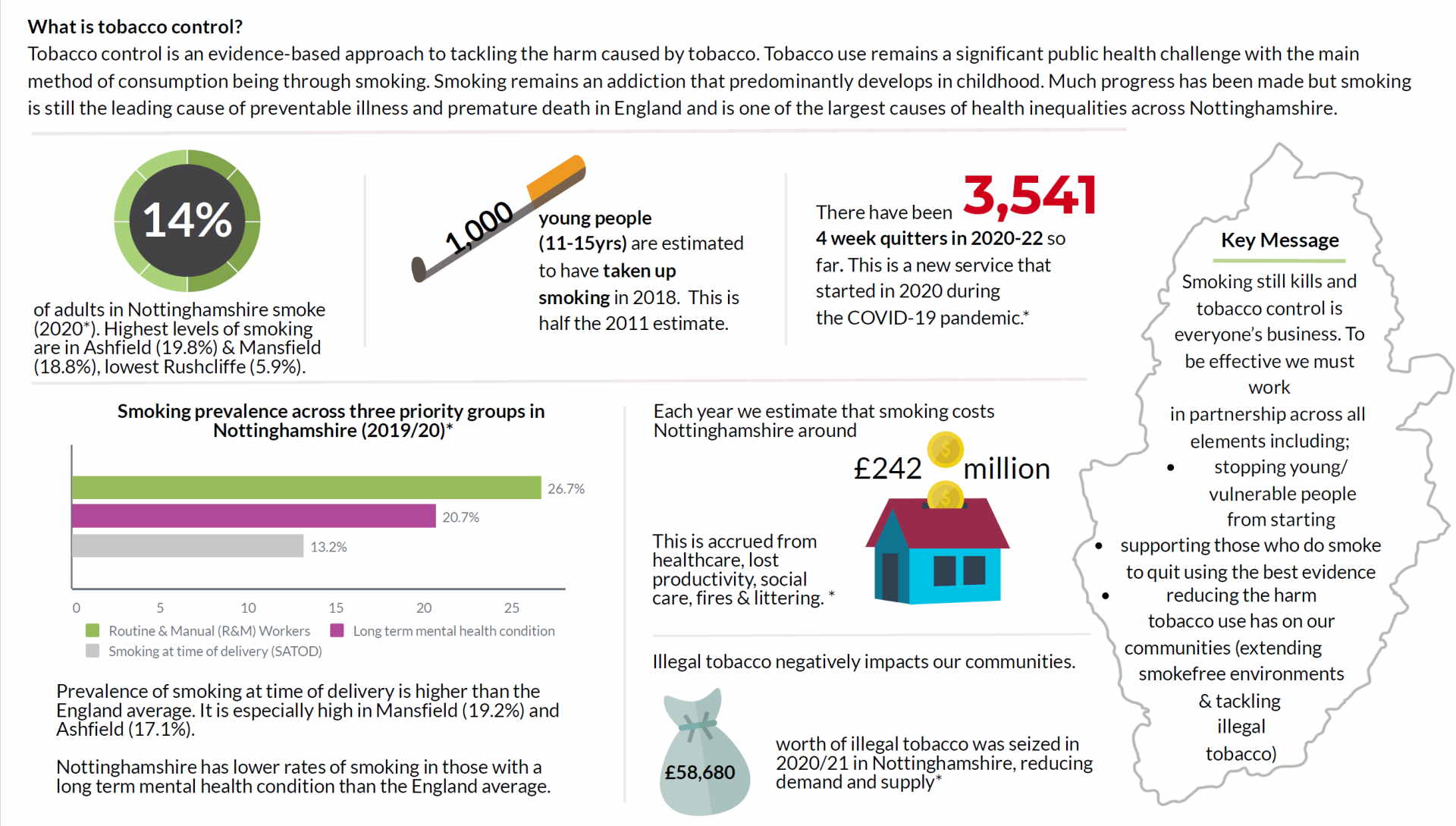
Infographic
Download infographic as PDF
Introduction
Tobacco use remains a significant public health challenge. The main method of tobacco consumption is through smoking. Smoking is still the leading cause of preventable illness and premature death in England; in 2016, around 78,000 were attributable to smoking in the UK, representing 16% of all deaths1.
Smoking causes harm to the heart (doubles the risk of a heart attack), the lungs (causes 84% of lung cancer and 83% of COPD deaths) and the brain (increases the risk of stroke by at least 50%) amongst many other health impacts1.
Smoking also has a significant financial impact, costing the country approximately £12.5bn per year, including £2.4bn to the NHS and £8.9bn from lost productivity2.
The percentage of people who smoke in Nottinghamshire is 15.4%, above the current England average and varies widely across the county- rising to 23.1% in Mansfield and 3.6% in Rushcliffe.
Smoking prevalence is higher amongst certain groups, such as routine and manual (R&M) workers (26.7%), people with serve mental illness (40.5%) and contributes to social inequalities (R&M workers in Newark and Sherwood are more than 6 times more likely to be a smoker than the rest of the population). Nottinghamshire also continues to have a higher rate of smoking during pregnancy than the England average (14.7% vs 10.8%)3.
This chapter is a refresh of the 2015 Tobacco chapter. It considers all forms of smoking and tobacco consumption, alternate methods of nicotine delivery, such as e-cigarettes and the wider effects of tobacco upon the community, across all ages and takes into account the wider determinants of health. The smoking of illicit substances is out of scope and considered separately in Substance Misuse: Young people and adults (2018) .
Notable changes in Nottinghamshire since the previous JSNA was published include;
- In April 2016 Smokefree life Nottinghamshire run by Solutions 4 Health became the new provider for Nottinghamshire’s stop smoking service.
- Smokefree polices have been implemented across all prisons nationally
- There has been a national increase in the use of e-cigarettes as an aid to quitting smoking with a better understanding of associated health risks.
- The development of the Integrated Care System (ICS), Integrated Care Partnerships (ICPs) and Primary Care Networks (PCNs).
A summary of the responses to the preceding assessment can be found in appendix 1.
Unmet needs and gaps - What we still need to improve
Stopping smoking
- a stop smoking approach that takes into account different personal factors such as age, sex, sexual orientation, ethnicity, level of education, mental health, levels of motivation and previous quitting methods or attempts
- services or support that is widely known, easily accessible and with as fewer barriers as possible
- the need to focus on geographical inequalities in smoking prevalence, with districts such as Ashfield, Newark and Sherwood and Mansfield having a much greater smoking prevalence than the rest of the county.
- the ongoing social inequalities in smoking prevalence which require equalising, particularly affecting groups such as R&M workers and those with a mental health condition.
- the ongoing challenges with smoking in pregnancy- the Nottinghamshire smoking at time of delivery (SATOD) rate is significantly worse than the England average
- the utilisation of popular novel technologies, such as e-cigarettes, as an adjunct to Nicotine Replacement Therapy (NRT) and behavioural support to help people to quit smoking.
- the links between stop smoking services and other lifestyle services, particularly those that may play a role in relapse prevention.
Preventing uptake
- evaluation of early-intervention programmes, such as ASSIST
- to reach more young people through social media awareness campaigns around the dangers of tobacco and the benefits of being smoke-free that are tailored to acknowledge the variations in local populations.
Reducing harm from tobacco use
- the demand and supply of illegal tobacco and be aware of the potential for the supply of newer counterfeit products, such as e-cigarettes
- a harm reduction approach, as specified in NICE guidance, for those who are unwilling to stop smoking or unable to stop completely, enabling the stop-smoking service to reach further into the smoking population
- enforcement of existing legislation designed to protect others from second-hand smoke (e.g. the ban on smoking in private vehicles with under-18s present).
- supporting the promotion and dissemination of guidance on safer smoking practices
- embedding routine brief advice on smoking and a healthy conversation approach across Nottinghamshire
- consistent knowledge and information on partner organisations work that supports the tobacco declaration
- supporting mechanism that allow for tobacco control activity to be planned and implemented across Nottinghamshire.
Recommendations for consideration
Recommendations |
Lead Organisations |
||||
| Local Authority | Service Providers | District & Borough Councils | Others | ||
|---|---|---|---|---|---|
Overall Tobacco Control Approach |
|||||
|
1 |
An approach that; |
||||
|
· targets the communities in which smoking prevalence is highest |
X | X | X | ||
|
· engages further with known priority groups, such as young people, pregnant women and R&M workers in order to address smoking inequalities |
X | X | |||
|
· engages with ‘at-risk’ groups not currently targeted, such as the LGBT community, certain ethnicities and other minority groups |
X | X | |||
· addresses the challenge of reducing smoking prevalence in those suffering from a mental health condition. |
X | X | |||
| 2 |
Informed future commissioning arrangements through understanding local in-depth insights in to the local population |
X | X | X | X |
Stopping Smoking |
|||||
| 3 |
A clear position guided by current evidence in the use of e-cigarettes as an effective quit method and to understand any cultural influences on their use |
X | X | ||
| 4 |
Ensure support/services are evidence-based, widely known and are easily accessible, with as fewer barriers as possible |
X | X | ||
Preventing the Uptake |
|||||
| 5 |
Understand the impact of the ASSIST peer led programme locally |
X | X | ||
| 6 |
Understand the role for wider evidence-based prevention programmes across the county |
X | |||
Reducing harm for Tobacco use |
|||||
| 7 |
Locally self-assess work on a broad range of tobacco control issues through; · Evaluating local action on tobacco control · ensuring that local activity follows the latest evidence-based practice · identifying priority areas for development and help with effective planning · monitoring improvements to services over time |
X | X | X | X |
| 8 |
Target those that trade in illegal tobacco |
X | X | X | |
| 9 |
Continue to support efforts to reduce the harm from tobacco use through; · Mass media campaigns · Extending smokefree environments · Supporting and enforcing current and emerging legislation · Safer smoking practices for those who continue to smoke |
X | X | X | X |
NB – services providers includes but not limited to local stop smoking services, trading standards, acute, maternity and mental health trusts, primary care, youth services
Others includes but not limited to Nottinghamshire fire and rescue service, ICS and ICP partners, Nottingham University, PHE, HMRC
Key contacts
This is an online synopsis of the topic which shows the executive summary and key contacts sections. To view the full document, please download it.